
The ICD-10 code for a tick bite is W57.XXXA — Bitten or stung by nonvenomous insect and other nonvenomous arthropods, initial encounter.
This external cause code classifies the tick bite exposure on the claim and pairs with the appropriate CPT code to describe what was done during the visit.
There is no ICD-10 code specifically labeled “tick removal” — the ICD-10 side describes why the patient presented, while the CPT side describes what the provider did.
The billing complexity in tick encounters isn’t the ICD-10 code itself — it’s deciding whether the tick removal qualifies for a separate procedural CPT code or falls within the evaluation and management (E/M) visit.
Most simple tick removals are included in the E/M service and are not separately billable. Only when the removal requires incision into subcutaneous tissue (foreign body extraction) do separate CPT codes like 10120 or 10121 apply.
In this guide, we’ll be exploring:
- The correct ICD-10 codes for tick bites, tick exposure, and tick-borne diseases
- When tick removal is separately billable vs included in the E/M visit
- Documentation requirements and common billing mistakes
- CPT code selection for simple vs complex tick removal
- Clinical scenarios with correct code pairings
Which ICD-10 codes apply to tick encounters?
Tick-related encounters use different ICD-10 codes depending on the clinical situation — uncomplicated bite, tick-borne disease, or post-removal follow-up. The code selected must match the documented reason for the visit.
Uncomplicated bite or sting by nonvenomous arthropod. Most common code for tick exposure without infection.
Follow-up visit for previously treated tick bite. Used when patient returns for monitoring.
Use when Lyme disease is confirmed or strongly suspected. Do not assign without clinical evidence.
Spotted fever due to Rickettsia rickettsii. Assign only with confirmed or suspected clinical diagnosis.
Use when the bite site develops localized infection without systemic tick-borne disease.
Use when clinical documentation supports infestation rather than a single bite exposure.
The encounter extension (A, D, or S) on W57 codes is required and changes the billing context. “A” (initial encounter) applies to the first visit for the tick bite. “D” (subsequent encounter) applies to follow-up visits for the same bite. “S” (sequela) applies when the patient presents with a late effect of the original tick bite.
For Lyme disease specifically, ICD-10-CM provides additional specificity beyond A69.20 — A69.21 (meningitis due to Lyme disease), A69.22 (other neurological disorders), and A69.23 (arthritis due to Lyme disease).
These codes should only be assigned when the corresponding complication is clinically documented, not presumed from the tick bite alone.
A coding error identified in many existing tick bite billing guides — some resources list B87.81 as a tick-related ICD-10 code.
This is incorrect.
B87 codes cover myiasis (fly larvae infestation), not tick-borne conditions. Loiasis (a parasitic infection sometimes mentioned in tick bite contexts) is properly coded under B74.3, and it is transmitted by deerflies, not ticks.
When is tick removal separately billable?
This is the decision that determines whether the encounter generates one claim line (E/M only) or two (E/M plus procedure).
No incision required
Minimal complexity
Bill E/M code only (99212–99215)
Most tick removals fall here
Incision required for extraction
Complex foreign body removal
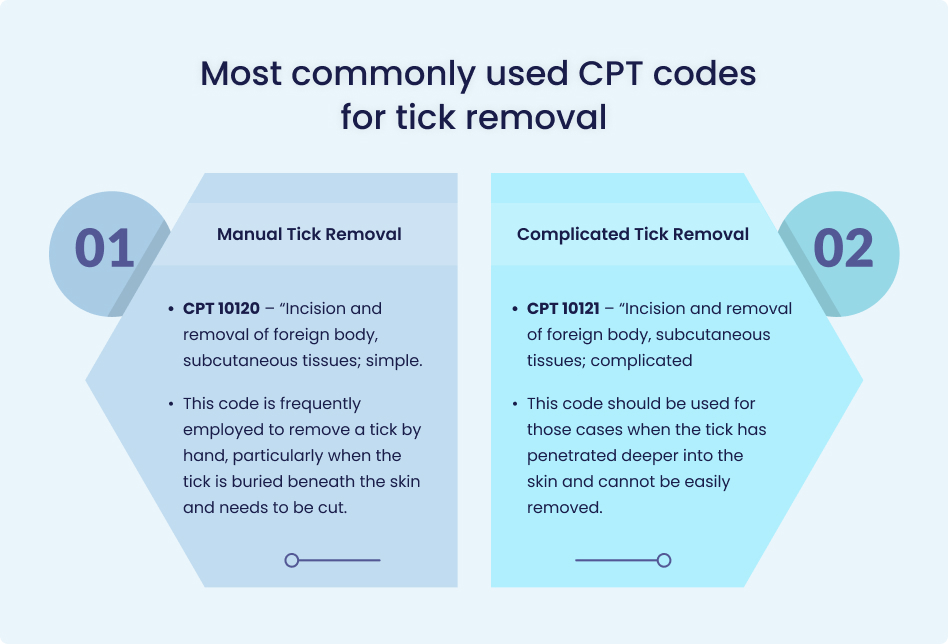
Bill CPT 10120 (simple) or 10121 (complicated)
Requires clinical documentation supporting complexity
The most common tick removal billing error — billing CPT 10120 or 10121 for every tick removal regardless of complexity. These codes describe incision and removal of a foreign body from subcutaneous tissue, not surface-level tick extraction with forceps.
If the provider simply grasped the tick with tweezers and pulled it out without cutting into tissue, the removal is part of the E/M visit. Billing 10120 for a surface removal that required no incision overstates the procedure and creates audit exposure.
CPT 10120 (simple foreign body removal) applies when the tick is deeply embedded and the provider must incise into subcutaneous tissue to extract it.
CPT 10121 (complicated foreign body removal) applies when the extraction involves exploration, deeper tissue dissection, or unusual complexity. Both codes require operative notes documenting the incision, depth of tissue involvement, and extraction technique.
When billing a separate procedure alongside an E/M visit on the same day, modifier 25 must be appended to the E/M code to indicate a significant, separately identifiable evaluation beyond the procedure itself.
Without modifier 25 and supporting documentation, NCCI edits will bundle the E/M into the procedure payment.
What do correct tick encounter billing scenarios look like?
Simple tick bite, tick removed at surface
A patient presents with a tick attached to the upper arm. The provider removes the tick with forceps, inspects the site, assesses for signs of infection, counsels the patient on Lyme disease symptoms to watch for, and documents the encounter.
- ICD-10: W57.XXXA
- CPT: 99213 (established patient E/M, low-moderate complexity)
- No separate procedure code — removal is part of the E/M service
Embedded tick requiring incision
A patient presents with a tick deeply embedded in the posterior scalp. The provider anesthetizes the area, makes a small incision, extracts the tick and surrounding tissue, irrigates the wound, and closes with adhesive strips.
- ICD-10: W57.XXXA
- CPT: 10120 (incision and removal of foreign body, simple)
- CPT: 99213-25 (E/M with modifier 25 if separately identifiable evaluation documented)
Tick bite with suspected Lyme disease
A patient returns two weeks after a tick bite with expanding erythema migrans rash and fever. The provider evaluates, orders Lyme serology, and initiates antibiotic therapy.
- ICD-10: A69.20 (Lyme disease, unspecified)
- CPT: 99214 (established patient E/M, moderate complexity)
- No tick removal code — the tick was removed at the initial encounter
Follow-up visit after tick removal
A patient returns for wound check one week after surgical tick removal. No new complaints, wound healing normally.
- ICD-10: W57.XXXD (subsequent encounter) or Z48.89 (encounter for other specified aftercare)
- CPT: 99212 (established patient E/M, straightforward)
What documentation prevents tick encounter claim denials?
Tick encounter documentation must support both the diagnosis code and the level of service billed.
Every tick encounter note should include the location of the tick on the body, whether the tick was attached or already partially removed, the removal technique used (forceps, incision, or other method), the clinical assessment of the bite site (signs of infection, erythema, edema), any counseling provided regarding tick-borne disease symptoms, and the plan for follow-up or testing if clinically indicated.
For encounters billed with CPT 10120 or 10121, the operative note must document the incision — that the provider cut into tissue to access the embedded tick.
Notes that describe only surface removal with forceps will not support a foreign body removal code, and a payer audit will downcode the claim to the E/M visit only.
For Lyme disease coding, documentation must support the diagnosis — clinical findings (erythema migrans, systemic symptoms), lab orders, or confirmed test results.
Assigning A69.20 based solely on a tick bite without clinical evidence of Lyme disease produces a CO-50 (medical necessity) denial because the diagnosis doesn’t support the encounter reason.
What tick encounter billing mistakes cause denials?
Some errors can cause denial:
No incision was performed. The removal was part of the E/M visit. Billing a foreign body removal code without incision documentation = upcoding.
Coding A69.20 for a tick bite exposure when no signs of Lyme disease are present. Produces CO-50 medical necessity denial.
W57.XXXA vs W57.XXXD vs W57.XXXS. Wrong extension = wrong encounter context. Payer edits reject the mismatch.
Billing E/M alongside 10120 without modifier 25 bundles the visit into the procedure payment. NCCI edit triggers CO-97.
B87 codes cover myiasis (fly larvae), not tick bites. Some billing guides incorrectly list B87.81 for tick encounters.
Accurate tick encounter billing starts with the right coding decision
Tick bite coding combines ICD-10 diagnosis selection, CPT procedure-level determination, and honest assessment of whether the removal complexity justifies a separate procedure code.
Most tick removals are simple, included in the E/M visit, and don’t warrant CPT 10120 — and billing them as if they do creates audit exposure that compounds across every tick encounter during peak season.
MedHeave operates as an embedded revenue cycle department inside medical practices, with AAPC-certified coders who validate ICD-10/CPT pairing, assess procedure complexity against documentation, and check NCCI bundling rules on every claim before submission.
- Claims submitted within 24–48 hours of signed encounter notes
- Denials addressed within 72 hours with payer-specific appeal templates
- Dedicated account managers with direct access (Monday–Friday, 9–5 EST)
- 90%+ first-pass rate across all claim types
- No lock-in agreements — 30-day exit, performance-based pricing (4–7%)
If coding accuracy and denial prevention are affecting your urgent care or primary care collections, contact MedHeave to see how structured billing closes those gaps.
Frequently asked questions
Here are some commonly asked questions on this topic:
W57.XXXA — Bitten or stung by nonvenomous insect and other nonvenomous arthropods, initial encounter — is the standard ICD-10 code for an uncomplicated tick bite. The “A” extension indicates the initial encounter. For follow-up visits related to the same tick bite, use W57.XXXD (subsequent encounter). If tick-borne disease (Lyme, RMSF) develops, the disease-specific ICD-10 code replaces or supplements the exposure code.
There is no single CPT code designated for “tick removal.” Most tick removals are included in the E/M visit (99212–99215) because they involve surface extraction with forceps and don’t require a separate procedure. CPT 10120 (incision and removal of foreign body, simple) applies only when the tick is embedded in subcutaneous tissue and the provider must incise to extract it. CPT 10121 applies to complicated extractions requiring deeper tissue exploration.
No. CPT 10120 describes incision and removal of foreign body, subcutaneous tissues, simple. The code requires documentation of an incision into tissue to access the embedded object. Surface tick removal with forceps or tweezers — without cutting into tissue — does not qualify for 10120 and should be reported within the E/M service. Billing 10120 without incision documentation creates upcoding risk and audit exposure.
Code Lyme disease (A69.20 or more specific A69.2x codes) only when clinical evidence supports the diagnosis — erythema migrans rash, systemic symptoms (fever, fatigue, joint pain), positive serology, or strong clinical suspicion documented by the provider. A tick bite alone, without signs or symptoms of Lyme disease, uses W57.XXXA (tick bite exposure). Premature assignment of Lyme disease codes without clinical findings produces medical necessity denials.
Routine tick removal generally does not require prior authorization. The procedure is considered an acute, low-complexity encounter that falls within standard outpatient coverage. Related services — such as Lyme disease laboratory testing, prophylactic antibiotic prescriptions, or follow-up imaging — may have coverage verification requirements depending on the payer. Check the patient’s specific plan benefits rather than assuming universal authorization rules.
B88.0 covers other acariasis — tick or mite infestation beyond a single bite exposure. This code applies when clinical documentation supports an infestation scenario (multiple ticks, parasitic burden) rather than an isolated bite. For a standard single-tick encounter, W57.XXXA is the correct code. B88.0 should only be assigned when the clinical situation describes infestation specifically.
