
InterQual criteria are proprietary, evidence-based clinical guidelines that healthcare organizations use to evaluate medical necessity and determine the appropriate level of care for patients.
Owned by Optum, InterQual supports admission reviews, observation status decisions, continued stay evaluations, post-acute placement, behavioral health level-of-care reviews, and prior authorization for imaging and procedures.
Payers, hospitals, and government agencies rely on these criteria during utilization review to match clinical documentation against standardized benchmarks.
Here is what the rest of this guide covers:
- Who uses InterQual criteria and why
- How criteria affect inpatient vs observation status
- What happens when a case does not meet criteria
- How the review workflow moves from request to decision
- A documentation checklist for providers preparing for review
- What severity of illness and intensity of service mean in practice
Who uses InterQual criteria?
InterQual criteria touch nearly every part of the utilization management workflow, from the initial admission review through discharge planning and care transition.
The primary users include:
- Payer review teams evaluating prior authorization requests
- Physician advisors who review cases that fail first-level screening
- Hospital revenue cycle teams tracking denial patterns tied to medical necessity
- Behavioral health reviewers assessing level-of-care placement for psychiatry + substance use
- Case managers coordinating care transitions and post-acute placement
- Medical directors issuing final determinations on escalated cases
- Utilization review nurses who screen cases against criteria
Optum reports that more than 4,300 hospitals and 300 payers and government entities currently use InterQual for clinical decision support.
In practice, the people who interact with InterQual criteria most frequently are UR nurses and case managers.
The quality of their review depends almost entirely on what the clinical documentation contains (which is something many providers don’t fully realize until a case gets denied).
What types of care do InterQual criteria cover?
InterQual spans medical, surgical, and behavioral health decisions across multiple care settings.
The criteria apply to
- Home care
- Pediatric acute care
- Long-term acute care
- Continued stay review
- Acute inpatient admissions
- Imaging and procedures requiring prior authorization
- Behavioral health (adult, geriatric, child, adolescent, substance use)
- Skilled nursing facility placement
- Ambulatory care planning
- Inpatient rehabilitation
- Discharge readiness
- Observation status
Optum’s InterQual portfolio includes Level of Care, Behavioral Health, and Ambulatory Care Planning content areas, along with specialty and industry-specific modules.
Several payer notices — from Independence Blue Cross to BCBSM — confirm InterQual is actively applied across acute care, pediatric, long-term acute care, home care, imaging, and behavioral health review.
How do InterQual reviews work?
A utilization review follows a predictable sequence, but the outcome depends heavily on how well the clinical record documents the patient’s condition and treatment needs.
UTILIZATION REVIEW WORKFLOW
How an InterQual review moves from request to decision
Request triggers review
Admission, continued stay, procedure, imaging, or post-acute placement
Criteria subset selected
Based on diagnosis, care setting, patient age, and service type
Documentation matched to criteria
Symptoms, vitals, labs, imaging, failed treatments, functional limitations, comorbidities
Criteria met or escalated
Approved at first-level review, or moved to physician review, peer-to-peer, or appeal
The reviewer identifies the relevant InterQual criteria subset based on diagnosis, care setting, patient age, and service type.
Clinical data is then pulled from the medical record — symptoms, vitals, lab values, imaging findings, failed treatments, functional limitations, and comorbidities — and each element is matched against the applicable criteria.
If the documented findings meet criteria, the case may be approved at first-level review.
If not, it moves to a secondary physician review, a request for additional documentation, or a peer-to-peer discussion between the treating and reviewing physicians.
A common mistake is assuming that if a patient needs care, the case will automatically meet criteria.
In practice, a medically reasonable case can fail first-level screening because the clinical documentation doesn’t capture the right details in the right places.
The care might be appropriate, but the record doesn’t prove it.
What are severity of illness and intensity of service?
Two concepts sit at the center of most level-of-care decisions. Severity of illness (SI) measures how clinically unstable or at-risk the patient is. Intensity of service (IS) measures the level of monitoring, treatment, and resources the patient requires.
| Question | Severity of illness | Intensity of service |
| What does it evaluate? | Patient condition and clinical risk | Care, treatment, and monitoring needed |
| Why does it affect the review? | Shows whether the patient is unstable enough for the requested setting | Shows whether the treatment plan justifies that level of care |
| Common documentation | Vitals, symptoms, labs, imaging, comorbidities, risk factors | Medication routes, monitoring frequency, procedures, nursing intensity |
When UR nurses apply InterQual criteria, they are essentially asking two questions at once — Is the patient sick enough? and Does the treatment plan require this level of care?
Both answers need to show up in the chart, supported by objective clinical indicators rather than vague summary statements.
For most UR teams, the tricky part isn’t identifying severity or treatment intensity in real time.
It’s finding that information documented clearly enough in the medical record to satisfy a retrospective criteria check.
How does InterQual affect inpatient vs observation status?
The observation-versus-inpatient decision is one of the most frequent and most contested applications of InterQual criteria in hospital settings.
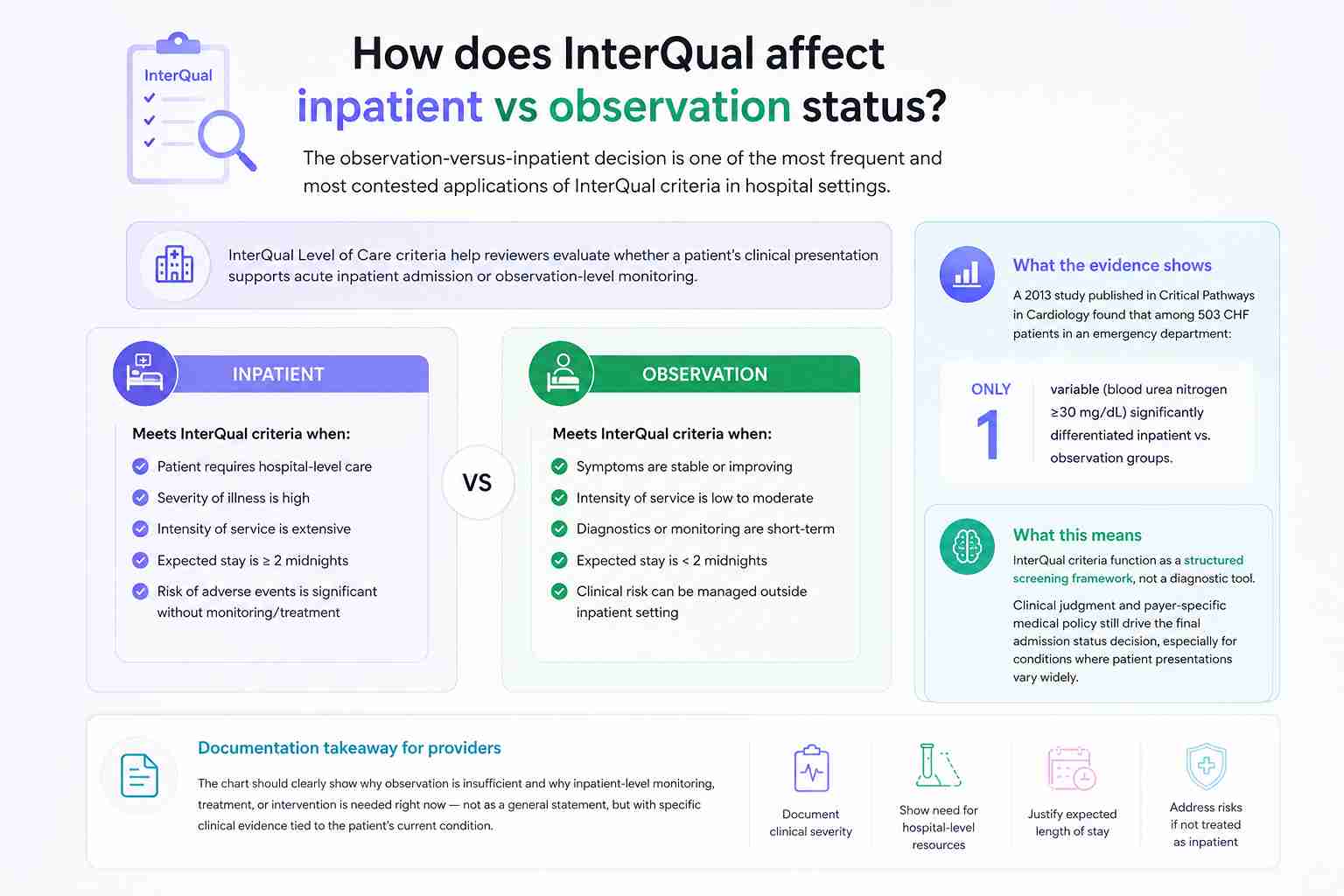
InterQual Level of Care criteria help reviewers evaluate whether a patient’s clinical presentation supports acute inpatient admission or observation-level monitoring.
A 2013 study published in Critical Pathways in Cardiology found that among 503 CHF patients in an emergency department, initial InterQual variables did not accurately predict level of care — only one variable (blood urea nitrogen ≥30 mg/dL) significantly differentiated the two groups.
The finding reinforces something experienced UR teams already recognize. InterQual criteria function as a structured screening framework, not a diagnostic tool.
Clinical judgment and payer-specific medical policy still drive the final admission status decision, especially for conditions where patient presentations vary widely.
For providers, the practical takeaway is documentation-focused.
The chart should clearly show why observation is insufficient and why inpatient-level monitoring, treatment, or intervention is needed right now — not as a general statement, but with specific clinical evidence tied to the patient’s current condition.
What happens when a case does not meet InterQual criteria?
Failing first-level criteria review does not mean the patient doesn’t need care.
It means the documented record, as reviewed against the applicable criteria set, did not meet the threshold for the requested level of care.
BY THE NUMBERS
The scale of utilization review decisions
4,300+
Hospitals using InterQual criteria
52.8M
MA prior auth determinations in 2024
7.7%
Of determinations denied in full or part
80%+
Of appealed denials overturned
Sources — Optum InterQual Overview (2024), KFF Medicare Advantage Prior Authorization Report (2026)
From the point of non-match, several paths exist
- The reviewer requests additional clinical documentation
- A physician advisor or medical director reviews the case
- A peer-to-peer discussion between the treating physician and the reviewing physician takes place
- The provider submits a formal appeal
KFF found that Medicare Advantage insurers made 52.8 million prior authorization determinations in 2024.
Payers denied 4.1 million (7.7%) in full or in part, yet only 11.5% of those denials were appealed. More than 80% of appealed denials were later overturned.
The overturn rate tells a clear story. Many denials stem from missing documentation rather than inappropriate care.
For revenue cycle teams, the most efficient denial prevention strategy starts before the initial review — with documentation that anticipates what a reviewer needs to see.
How do InterQual and MCG compare?
InterQual (Optum) and MCG are the two dominant proprietary clinical criteria tools in utilization management.
Both are evidence-based, both support medical necessity decisions, and both serve payers, hospitals, and government programs.
| Area | InterQual | MCG |
| Primary function | Criteria-based medical necessity and level-of-care review | Evidence-based care guidelines and utilization review |
| Common users | Payers, hospitals, health systems, government entities | Payers, hospitals, government entities |
| Practical reviewer focus | Matching documented findings to specific clinical criteria elements | Matching care needs to expected care pathways and recovery timelines |
| Access | Licensed, proprietary | Licensed, proprietary |
| Often described as | More granular and condition-specific | More pathway-oriented and recovery-focused |
Some UR nurses describe InterQual as more detailed in its clinical element matching, while MCG tends to orient reviewers toward care progression and expected length of stay.
Optum describes InterQual as evidence-based clinical decision support for appropriate utilization, while MCG describes its care guidelines as evidence-based and regularly updated.
The real difference often depends on how a specific payer or health system has implemented and configured the tool — not on any inherent superiority of one over the other.
Providers working with multiple payers will likely encounter both, and the documentation principles remain largely the same regardless of which tool the reviewer is using.
Can you access InterQual criteria online?
Full InterQual criteria are proprietary and not available as a free public resource. Access typically comes through an employer, payer, hospital, health system, or licensed platform.
Most credentialed users log in through One Healthcare ID, Optum’s authentication portal, or through a payer-specific system.
Some organizations access InterQual through integrated utilization management software or platforms like Availity.
Providers searching for “InterQual criteria PDF” should be cautious.
Downloaded criteria from unofficial sources may be outdated, incomplete, or mismatched to the payer’s current version.
Payers implement updated InterQual versions on different schedules — Independence Blue Cross, for example, announced it would begin using 2025 InterQual Criteria on August 18, 2025, while BCBSND listed August 1, 2025.
Optum updates InterQual criteria annually through a structured development process involving peer review by more than 1,100 actively practicing physicians and clinicians. If a provider needs to see the specific criteria used in a coverage decision, most payer processes allow requesting the clinical rationale or criteria basis for that determination.
How can providers document for InterQual review?
Strong clinical documentation is the single most controllable factor in whether a case meets InterQual criteria.
Reviewers can only match what appears in the chart — and a patient’s actual clinical picture is irrelevant to the review if the record doesn’t reflect it.
A defensible medical record for utilization review should include
- Barriers to discharge or safe transition
- Treatment intensity and monitoring requirements
- Daily progress updates during continued stay review
- Current symptoms and their functional impact on the patient
- What lower-level care was attempted, and why it would be unsafe
- Objective findings (vitals, labs, imaging, exam results)
- Why care is needed now rather than at a later date
- Comorbidities that increase clinical risk
| Weak documentation | Stronger documentation |
| “Patient needs admission.” | “Patient requires inpatient monitoring due to persistent hypotension unresponsive to IV fluids.” |
| “Failed outpatient care.” | “Completed 10-day oral antibiotic course with worsening symptoms and new imaging findings.” |
| “Needs rehab.” | “Requires daily skilled PT/OT due to measurable decline in mobility and ADL independence post-hip fracture.” |
The biggest documentation gap most teams face isn’t missing information — it’s clinical reasoning that exists in the provider’s head but never makes it into the written record.
A reviewer three states away cannot evaluate what was never documented, and by the time the denial arrives, the opportunity for real-time documentation improvement has passed.
When utilization review decisions affect your revenue
Medical necessity denials tied to InterQual criteria create real financial pressure for practices — especially when documentation gaps are the root cause.
MedHeave helps healthcare providers strengthen their revenue cycle by connecting clinical documentation to billing and authorization workflows.
- Revenue recovery for improperly denied claims
- Denial pattern analysis tied to payer-specific criteria
- Documentation improvement support for UR-related claims
- Prior authorization management across medical and behavioral health services
Contact MedHeave to see how your practice can reduce criteria-related denials and protect revenue.
Frequently asked questions
Here are some commonly asked questions on InterQual criteria:
InterQual criteria points are the specific clinical elements a reviewer checks against the patient record when applying a given criterion. Each point represents a documented finding — a symptom, vital sign, lab result, failed treatment, functional limitation, or treatment intensity indicator — that either supports or does not support the requested level of care. Points are not a public scoring system with numeric values. They function more like a checklist of clinical data elements that the medical record needs to contain to meet the criteria threshold for a specific care setting or service.
Not necessarily. A case that does not meet InterQual criteria at first-level review may simply have incomplete documentation, or the patient’s clinical situation may require physician-level judgment beyond what the screening criteria capture. The case can be escalated to a physician advisor, reviewed through peer-to-peer discussion, or formally appealed. InterQual criteria support the utilization review process, but they do not replace clinical decision-making or override payer-specific medical policies, Medicare regulations, or state-level requirements that may also apply to the coverage decision.
Yes. InterQual includes behavioral health criteria covering adult and geriatric psychiatry, child and adolescent psychiatry, substance use disorders, and behavioral health services. Reviewers assess risk of harm, functional status, treatment history, environmental stressors, and engagement in care. Optum’s behavioral health content areas also address parity compliance, comorbidities, social determinants of health, and transition planning. For substance use disorder reviews, InterQual can work alongside ASAM-related tools within utilization review workflows to support level-of-care placement decisions.
Optum updates InterQual criteria annually through a structured evidence-based development process. Clinical development teams conduct systematic evidence reviews, and peer review panels of more than 1,100 actively practicing physicians and clinicians evaluate the criteria before release. Payers then implement updated versions on their own schedules, which means the same year’s criteria may go live at different times depending on the health plan. Providers should verify which criteria version their payer is currently using, especially during the transition window between annual releases.
No. InterQual criteria support the medical necessity review process, but payer policies, plan-specific benefit rules, Medicare regulations, state mandates, and contractual terms may also affect coverage decisions. A case could meet InterQual criteria and still face a denial based on benefit exclusions or policy limitations. Conversely, a case that does not meet InterQual screening criteria may still be approved after physician review or appeal. Treating InterQual as the only rule governing coverage decisions is a frequent source of confusion for both providers and patients.
