The CO-16 denial code means the claim lacks information or has a submission/billing error that prevents the payer from processing it.
The official X12 CARC definition reads “Claim/service lacks information or has submission/billing error(s).” It falls under the CO (Contractual Obligation) group, which typically means the provider — not the patient — absorbs the financial adjustment.
CO-16 is not a clinical denial. It is also not a coverage denial. It is a data completeness failure — and one of the highest-volume denial codes across all specialties because it covers a broad range of missing or incorrect claim elements.
Here is what the rest of the article breaks down:
- Why CO-16 is useless without its remark code
- How CO-16 compares to CO-4, CO-97, and CO-109
- The five root causes that trigger most CO-16 denials
- Prevention strategies that stop CO-16 before it happens
- How to read the RARC to identify the actual problem
- Step-by-step workflow to resolve CO-16 denial
Why is CO-16 called a “wrapper code”?
CO-16 tells you that something is wrong with the claim. It does not tell you what is wrong.
The actual diagnostic information lives in the Remittance Advice Remark Code (RARC) attached to CO-16 on the ERA or EOB.
X12 standards require at least one RARC with every CO-16 adjustment. The RARC specifies the exact data element that failed — the missing modifier, the invalid NPI, the incorrect date of birth, the absent authorization number.
Without reading the RARC, a billing team looking at CO-16 alone is staring at a label that says “something is broken” with no indication of what.
A few common CO-16 + RARC pairings that appear across payer systems.
- CO-16 + N290 — missing or invalid provider identifier
- CO-16 + N382 — missing or invalid prior authorization number
- CO-16 + M51 — missing or incomplete procedure code information
- CO-16 + MA130 — claim lacks required information for adjudication
The RARC is the fix instruction. CO-16 is just the category. Billing teams that train staff to read the RARC first (before researching the denial) resolve CO-16 claims faster than teams that troubleshoot the code itself.
Stop treating every CO-16 denial the same way
MedHeave’s denial management team reads the remark code behind each CO-16 adjustment and traces recurring codes back to the workflow step that’s causing them.
What causes CO-16 denials?
Most CO-16 denials originate upstream — at registration, eligibility verification, or authorization — before the claim ever reaches the billing team. The claim data was incomplete or incorrect from the start, and no one caught it before submission.
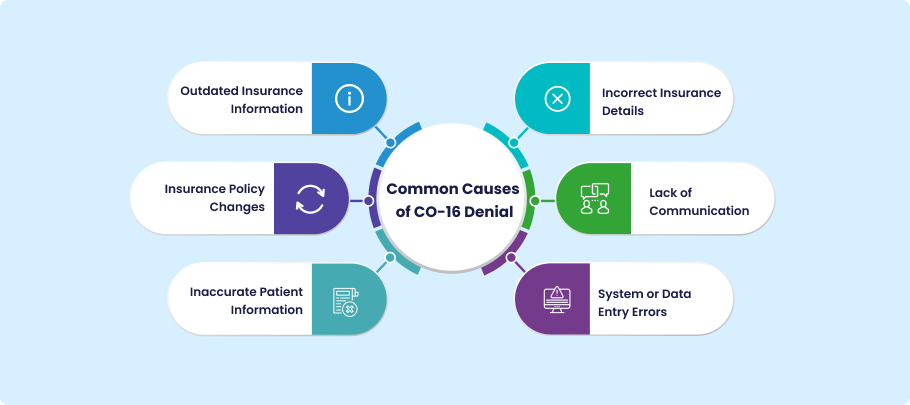
Five root causes account for the majority of CO-16 volume across both Medicare and commercial payers.
Provider data errors
An invalid or missing NPI, a taxonomy code that does not match the service billed, or a rendering/referring provider field left blank. CMS requires valid provider identifiers on every claim, and payer systems reject automatically when the provider data fails validation.
Patient demographic errors
A misspelled name, transposed digits in the date of birth, an incorrect gender code, or an outdated address.
Payer systems match claim demographics against enrollment records — a single character mismatch in the subscriber name or DOB can trigger CO-16 before the payer even looks at the procedure code.
Insurance and eligibility failures
An outdated member ID, a lapsed policy, or the wrong payer on the claim. When the insurance information captured at registration does not match the payer’s active enrollment file, the claim is rejected for missing or invalid coverage data.
Authorization gaps
A prior authorization number that was required but not included on the claim, or an auth that was obtained but for a different date of service or procedure code. The payer’s system flags the claim as lacking required information because the authorization field is empty or does not match.
Coding and modifier errors
A CPT code that requires a modifier (like -25 or -59) but the modifier was not appended, an ICD-10 code that has been deleted or does not support the procedure, or a CPT-ICD pairing that the payer’s edits do not accept. The claim has a billing error in the coding layer that the payer identifies as incomplete or invalid data.
How should billing teams resolve CO-16?
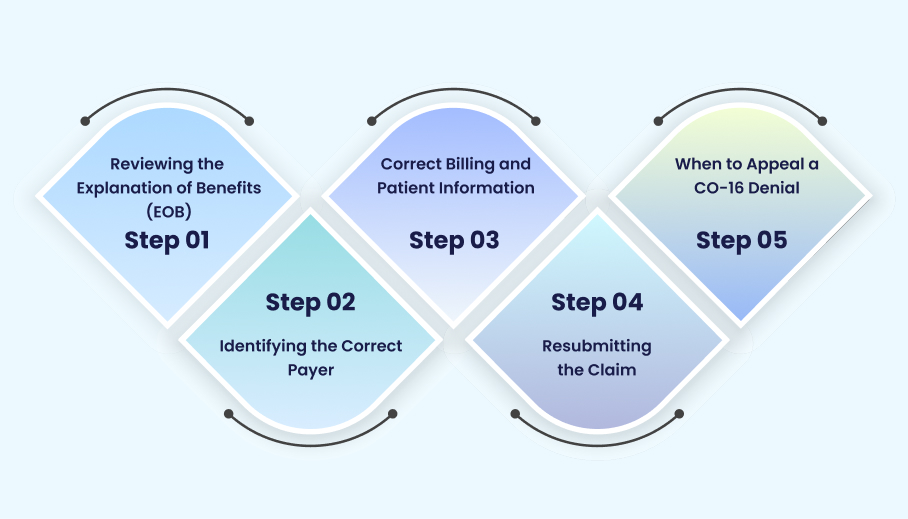
The resolution workflow for CO-16 follows a specific sequence. Skipping steps or guessing at the problem without reading the RARC produces wasted resubmissions that get denied again for the same reason.
Read the RARC first
Open the ERA (Electronic Remittance Advice) or EOB and identify the RARC attached to the CO-16 adjustment. The remark code tells you exactly which data element failed.
N382 means authorization. N290 means provider ID. MA130 means the claim is missing required information for adjudication. Start with the RARC — not with CO-16 itself.
Identify the failed data element
Map the RARC to the specific claim field. Provider data errors live in the NPI, taxonomy, or rendering provider fields.
Demographic errors live in the patient name, DOB, gender, or subscriber ID fields. Authorization errors live in the prior auth number field. Coding errors live in the CPT, ICD-10, or modifier fields.
Correct the claim
Fix the identified data element. Do not change anything else on the claim — additional edits introduce new variables that can trigger a different denial on resubmission.
Resubmit (not appeal)
CO-16 is almost always a corrected claim resubmission, not an appeal. Appeals are appropriate when you believe the payer made an error in adjudication.
CO-16 indicates the claim had a data problem — the fix is correcting the data and resubmitting. Resubmitting preserves the original filing date with most payers (check payer-specific rules), but the corrected claim must arrive before the timely filing deadline expires.
Track the pattern
If the same RARC appears across multiple CO-16 denials, the problem is systemic — not claim-specific.
A recurring N290 (invalid provider ID) suggests an enrollment gap. A recurring N382 (missing auth) suggests a front-desk workflow failure.
Fixing individual claims without addressing the pattern guarantees the same denials next month.
Resolution workflow
How to fix CO-16 — in order
CO-16 alone is a category, not a diagnosis. The remark code tells you *what* failed.
Provider NPI? Patient DOB? Missing modifier? The RARC points to the specific field.
Changing other fields introduces new variables. Fix what broke. Nothing else.
Not an appeal. CO-16 is a data problem, not an adjudication dispute. Correct and resubmit.
Same remark code across multiple claims = upstream workflow problem, not a one-time error.
How does CO-16 compare to other denial codes?
Billing teams frequently encounter CO-16 alongside other CO-group codes, and knowing which code applies determines the resolution path. A claim denied under CO-16 requires a different fix than one denied under CO-4 or CO-97.
| Denial code | Official meaning | Typical root cause | Resolution path |
| CO-16 | Claim lacks information or has billing errors | Missing data (demographics, NPI, auth, modifier) | Correct missing/invalid field, resubmit |
| CO-4 | Procedure code inconsistent with modifier or diagnosis | CPT-ICD mismatch, wrong modifier, bundling conflict | Review coding logic, fix modifier or diagnosis, resubmit |
| CO-97 | Payment included in another service/procedure | Bundled service billed separately | Check NCCI edits, remove duplicate or add modifier if distinct |
| CO-109 | Claim not covered by the payer identified | Wrong payer on claim, insurance routing error | Verify correct payer ID, resubmit to correct insurer |
| CO-197 | Precertification/authorization/notification absent | Prior auth required but missing | Obtain auth retroactively (if allowed) or submit proof of existing auth |
The critical operational difference is that CO-16 is a data completeness issue (something is missing or wrong on the claim form), while CO-4 is a coding logic issue (the codes do not make clinical or billing sense together), CO-97 is a bundling issue (the service is included in another code’s payment), and CO-109 is a routing issue (the claim went to the wrong payer entirely).
Treating all denial codes the same — sending every rejected claim through the same correction workflow — wastes time because each code has a different root cause and a different fix.
What makes CO-16 so expensive?
CO-16 is not a high-dollar denial per claim. A single CO-16 on a $150 office visit does not threaten the practice. The cost comes from volume and recurrence.
1. Rework consumes billing staff capacity
Because CO-16 covers a broad range of data issues, it occurs frequently. Each denial requires staff to identify the problem, correct the claim, and resubmit it, creating a significant administrative workload when repeated across hundreds of claims.
2. Delayed reimbursement increases A/R aging
The real financial damage is indirect. CO-16 denials increase accounts receivable aging, delay cash flow by restarting the payer’s adjudication timeline, and reduce clean claim rates through avoidable data-entry errors.
3. Denial trends expose front-end process failures
For practices that track denials by CARC, high CO-16 volume often reveals registration and eligibility weaknesses that appear to be billing problems but originate much earlier in the revenue cycle.
How do you prevent CO-16 before the claim ships?
Every CO-16 denial represents a data gap that existed before the claim was submitted.
The claim scrubber did not catch it, or there was no claim scrubber. The eligibility check was not run, or the results were not reviewed. The registration was incomplete, or no one verified it.
Prevention means closing those gaps before the claim leaves the building.
Eligibility verification at check-in
Real-time eligibility checks catch outdated insurance, lapsed coverage, and subscriber ID mismatches before the encounter is documented — and long before the claim is submitted.
Running eligibility only at scheduling (days or weeks before the visit) misses coverage changes that occur between scheduling and the appointment date.
Pre-submission claim scrubbing
Claim scrubbing tools validate required fields, check CPT-ICD pairings, flag missing modifiers, and verify provider identifiers before the claim is transmitted to the clearinghouse.
Claims that fail scrubbing are returned for correction internally — where the fix takes minutes — rather than denied by the payer, where the fix takes days or weeks.
Registration data audits
A quarterly audit of patient registration data accuracy — checking a sample of accounts for correct insurance, subscriber ID, DOB, and guarantor information — identifies patterns that front-desk staff can address through retraining or workflow changes.
Registration errors are habitual (the same error type repeats across staff and patients) and an audit catches the pattern that individual claim corrections do not surface.
Denial trend monitoring
Tracking CO-16 denials by RARC over time shows whether the same data failure is recurring.
A spike in N290 (provider ID) denials after a new physician joins the practice signals an enrollment gap. A steady volume of N382 (authorization) denials signals a front-desk authorization capture failure.
Trend data converts reactive denial management into proactive workflow correction.
Does CO mean the patient cannot be billed?
The CO (Contractual Obligation) group code generally indicates that the adjustment is the provider’s responsibility under the payer contract — meaning the provider writes off the amount rather than billing the patient.
However, patient billing responsibility is determined by the specific payer contract, the denial reason, and the circumstances of the claim. CO does not automatically prohibit patient billing in every situation.
In most CO-16 scenarios, the provider corrects the data error and resubmits the claim. The denied amount is not written off permanently — it is recovered through resubmission.
Patient billing only becomes relevant if the claim remains unpaid after all correction and appeal options are exhausted, and even then, contract terms govern whether the balance can shift to the patient.
The practical takeaway for billing teams is that CO-16 denials should be corrected and resubmitted — not written off and not billed to the patient as a first response.
Turn CO-16 from your top denial into a solved problem
CO-16 is one of the most preventable denial codes in medical billing because every cause is a data gap — and data gaps have data fixes. The challenge is not knowing what to do. The challenge is building the upstream controls that catch the problem before the claim ships.
- Verify eligibility at check-in, not just at scheduling
- Scrub every claim before submission (automated, not manual)
- Track CO-16 volume by RARC to identify systemic root causes
- Audit registration data quarterly to catch recurring entry errors
- Train front-desk and billing staff on the top five RARC codes they see most
Contact MedHeave to build CO-16 prevention into your billing workflow — and stop paying your staff to fix claims that should have been clean on the first pass.
Frequently asked questions
Here are some commonly asked questions on this topic:
CO-16 is a Claim Adjustment Reason Code (CARC) that means “Claim/service lacks information or has submission/billing error(s).” It indicates the payer could not process the claim because required data was missing, incorrect, or inconsistent. CO-16 always appears with a Remittance Advice Remark Code (RARC) that specifies which data element failed — the CO-16 code itself only identifies the category of error, not the specific problem.
The official X12/HIPAA definition of CO-16 is “Claim/service lacks information or has submission/billing error(s) which is needed for adjudication.” It falls under the CO (Contractual Obligation) group code, which generally means the provider — not the patient — is responsible for the adjustment. The RARC attached to CO-16 provides the specific denial reason (missing authorization, invalid NPI, incorrect demographics, etc.).
Start by reading the RARC on the ERA or EOB — the remark code identifies the exact data element that failed. Map the RARC to the corresponding claim field (provider NPI, patient DOB, missing modifier, authorization number). Correct the identified field and resubmit the claim as a corrected claim, not an appeal. CO-16 is a data problem, and the standard resolution is correction and resubmission within the timely filing window.
CO-16 fires when the payer’s system identifies missing, invalid, or incomplete data on the claim. The most common triggers are invalid or missing provider identifiers (NPI, taxonomy), patient demographic errors (DOB, name, gender), outdated insurance information (member ID, payer ID), missing prior authorization numbers, and coding errors (absent modifiers, invalid CPT-ICD pairings). The specific reason is always identified in the RARC that accompanies the CO-16 adjustment.
Identify the RARC, correct the failed data element, and resubmit the claim. Do not appeal CO-16 unless you believe the payer made an error in applying the code. If the same RARC appears across multiple CO-16 denials, the problem is systemic (enrollment gap, front-desk workflow failure, missing scrubbing rule) and requires an upstream process fix — not just claim-by-claim correction.
The CO group code generally indicates the adjustment is the provider’s contractual responsibility, not the patient’s. In most CO-16 situations, the provider corrects the data error and resubmits the claim — the amount is recovered through resubmission, not billed to the patient. However, patient billing rules depend on the payer contract and the specific circumstances. CO-16 denials should be corrected and resubmitted as the first response, not written off or transferred to the patient.
CO-16 indicates missing or incorrect claim data (a data completeness problem). CO-4 indicates the procedure code is inconsistent with the modifier used or the diagnosis reported (a coding logic problem). CO-16 is fixed by supplying missing data or correcting invalid entries. CO-4 is fixed by reviewing the CPT-ICD-modifier relationship and correcting the coding error. Both require resubmission, but the root cause and the troubleshooting path are different.
